Anthracyclines such as doxorubicin, daunomycin and darubicin belong to a class of chemotherapeutic drugs that is widely used to treat paediatric cancers. Advances in chemotherapy, other treatment strategies and supportive care have led to significant improvements in paediatric cancer outcomes, with current five-year survival rates exceeding 80%.
Improved survival rates mean that there are now more than 400,000 long-term childhood cancer survivors in the U.S, and this number is steadily growing. Remarkably, one quarter of all childhood cancer survivors living in the U.S. today have survived for more than 30 years following their diagnosis.
Improved survival is complicated
Although improved survival rates are a major step forward for childhood cancer, treatment-associated complications are a growing concern. While children generally tolerate the acute effects of chemotherapy relatively well compared to adults, exposure to chemotherapy, radiation, and/or surgery during childhood can contribute to serious complications that may not manifest until years after the completion of therapy.
Childhood cancer survivors have a greater than five-fold risk of developing heart failure compared to age-matched controls![]()
Recent studies revealed that two out of three childhood cancer survivors will develop a chronic health condition such as subsequent malignant tumours, cardiovascular problems, endocrine diseases, and musculoskeletal disorders. Of these, anthracycline-associated cardiovascular complications remain a leading cause of late mortality and morbidity in childhood cancer survivors. Today, those that survive childhood cancer have a five-fold greater risk of developing heart failure (HF) compared to age-matched controls, and the overall survival rate following these complications is less than 50%.
Anthracyclines and heart failure
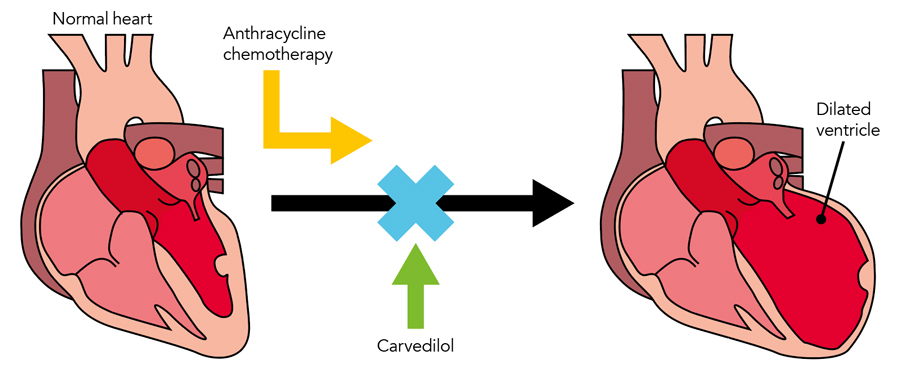
Cardiotoxicity resulting from anthracycline exposure occurs along a continuum from asymptomatic cardiac dysfunction characterised by abnormalities of cardiac function and structure detected via imaging studies, to clinically evident HF. Heart failure is initiated by the formation of free radicals, which leads to remodelling and weakening of the cardiac muscle, eventually impairing the heart’s ability to pump blood efficiently. The link between childhood anthracycline exposure and HF risk is dose-dependent. In other words, the greater the exposure to anthracyclines during childhood, the greater the risk of HF later in life.

The growing number of childhood cancer survivors makes it crucial that strategies are developed to prevent symptomatic heart disease in this vulnerable population. Dr Armenian’s research addresses the urgent need to prevent symptomatic heart disease in childhood cancer survivors in two ways – by preventing cardiovascular complications in at risk individuals, and by developing early screening tools to identify the individuals most at risk of anthracycline-related HF.
The PREVENT-HF clinical trial
Until recently, efforts to prevent cardiovascular complications in cancer survivors relied almost exclusively on primary prevention strategies such as dose reduction or avoidance of potentially cardiotoxic therapies. Examples of such strategies include: reducing the use of anthracycline-like drugs, alternative drug administration schedules, and co-administration of drugs that protect the heart (cardioprotectants). While these studies have been encouraging overall, most study participants had breast or other solid cancers, and few studies included children.
While dose reduction might be an effective preventative strategy in childhood cancers that have favourable outcomes such as Hodgkin lymphoma and acute lymphoblastic leukaemia, it is unrealistic for other malignancies such as certain musculoskeletal tumours, where anthracyclines remain the backbone of most treatment regimens. Given that around 240,000 long-term childhood cancer survivors are believed to already have been exposed to potential cardiotoxic therapies, primary prevention is not a viable one size fits all approach. The growing population of childhood cancer survivors now represents one of the largest new risk groups for preventable symptomatic heart disease in adulthood.
Dr Armenian is currently leading a large Phase IIB clinical trial (known as PREVENT-HF), which aims to investigate the potential to reduce HF risk in childhood cancer survivors by low-dose treatment with a cardioprotectant, carvedilol. Carvedilol is a third generation non-selective ß-blocker that lowers blood pressure and is capable of reversing structural changes to heart tissue following exposure to high dose anthracyclines.
The study, which is currently in the recruitment phase, involves 70 participating institutions from around the world, and is the first trial to systematically evaluate in a prospective manner the natural progression of chemotherapy-induced HF. The results are expected in 2022, and pending their outcome, they have the potential to change daily management and practice for the growing cohort of childhood cancer survivors.
Mobile health (mHealth)-based cardiac monitoring
In collaboration with California Institute of Technology, Dr Armenian is testing whether a novel mHealth platform can be used to monitor cardiac function in survivors at risk for developing HF. This innovative solution exploits the growing field of telemedicine, enabling childhood cancer survivors to check their heart health as regularly as they desire, and relay the information back to their doctors in real time.
This technology has the potential to change the day-to-day practice of clinicians caring for the >550,000 non-oncology patients diagnosed with heart failure each year![]()
When completed, this study will provide important information regarding the utility and accuracy of this platform to measure cardiac function, compared with the established standard of care (2D echocardiography) as well as a more costly yet accurate measure of cardiac systolic function (magnetic resonance imaging). This will in turn facilitate the development of population-based research in large cohorts of cancer survivors at a fraction of the cost and resources usually necessary to conduct such studies.
Importantly, once validated, this technology also has the potential to transform the daily practice of clinicians who care for the >550,000 non-oncology patients diagnosed with HF annually, allowing real-time monitoring and management of their heart disease without the lag-time between imaging and interpretation of results.
Two paths – one goal
Dr Armenian’s work is motivated by the necessity to explore multiple strategies to realise the urgent goal of reducing heart failure in childhood cancer survivors. The PREVENT-HF trial is the first of its kind to systemically investigate the potential of a cardioprotectant to reduce anthracycline-mediated heart failure in this cohort, while the mHealth-based cardiac monitoring platform is at the cutting edge of modern telemedicine. The achievements and advances in childhood cancer until now are a worthy cause for optimism, and time will tell whether Dr Armenian’s two-pronged approach will help to solve one of the significant remaining challenges in the childhood cancer field.
It is well-established that there is marked variability in the prevalence and severity of therapy-related HF that is not explained exclusively by clinical and treatment factors such as age at exposure, sex, and cumulative anthracycline dose. Studies are under way to examine how an individual’s genetic make-up could explain the variability in risk. The information obtained from these studies could set the stage for the development of accurate and personalised risk-prediction models, providing physicians and patients with knowledge about HF risk even before administration of therapy. This would allow them to avoid certain exposures, if a comparable alternative exists, or closely monitor patients during and after therapy.
Is the HF risk greater after certain types of cancer than others?
HF is more prevalent in individuals with certain cancers because of the intense treatment for cure, not because of the cancer itself.
Given the toxicity associated with anthracyclines, wouldn’t it make more sense to intensify efforts to avoid their use altogether, rather than finding ways to circumvent or counteract their toxicity?
It is important to note that the development of anthracyclines contributed to the tremendous cure rates we see today, and that the vast majority of children treated with anthracyclines do not develop HF. For many types of cancers, there are no alternatives to anthracyclines. As such, it is imperative to develop novel strategies for personalised delivery of these drugs, taking into consideration the genetic risk factors as well as the physical health of the patient at the time of treatment. Efforts are underway to develop less toxic therapies for both paediatric and adult cancer patients. It is the responsibility of the oncology community to translate the knowledge gained from our survivorship studies today towards better cures for tomorrow.
How accurate do you expect the mHealth-based platform to be in detecting cardiac dysfunction?
Our initial study of approximately 200 patients showed that the handheld mHealth platform was as accurate as cardiac magnetic resonance imaging (MRI), which is the gold standard measure of heart function. Additional validation studies are under way in both paediatric and adult populations, and should shed more light on the accuracy of this platform in oncology and non-oncology settings.
What’s next for your research?
With the advent of new integrative electronic health record systems, we have the opportunity to utilise advances in computer sciences (e.g., natural language processing) to study health outcomes in hundreds of thousands of patients at a fraction of the time it takes to study them today. This has the potential to not only capture health information more rapidly, but to share this knowledge with researchers and practitioners who are developing the next generation of therapeutic clinical trials. The challenge facing clinicians and researchers alike is how to integrate genomics, personalised medicine, and risk prediction into real-time decision making for our patients and families. These decisions have to be balanced by very real concerns such as the cost-effectiveness of our screening and treatment approaches. As such, we have a number of studies examining new paradigms in care delivery for our most vulnerable patients. As paediatric oncologists, we have to ensure that our patients not only survive their treatment, but thrive for decades afterwards, recognising that their best days are ahead of them.
Dr Armenian’s lab focuses on understanding and mitigating the risk factors involved in chemotherapy-associated cardiovascular complications in survivors of childhood and adult-onset cancer.
Funding
- National Institutes of Health (NIH)
- Leukemia and Lymphoma Society (LLS)
- American Cancer Society (ACS)
Collaborators
- Smita Bhatia, MD, MPH (www.uab.edu/medicine/icos/members/smita-bhatia)
- Pamela Douglas, MD (https://medicine.duke.edu/faculty/pamela-susan-douglas-md)
- Ming Hui Chen, MD, MSc (www.childrenshospital.org/doctors/ming-hui-chen)
- Morteza Gharib, PhD (http://eas.caltech.edu/people/mgharib)
Bio
 Dr Saro Armenian is an Associate Professor in the Departments of Pediatrics and Population Sciences, and the Director of the Division of Outcomes Research and the Center for Survivorship and Outcomes at City of Hope, a world leading research and treatment center in Los Angeles, California.
Dr Saro Armenian is an Associate Professor in the Departments of Pediatrics and Population Sciences, and the Director of the Division of Outcomes Research and the Center for Survivorship and Outcomes at City of Hope, a world leading research and treatment center in Los Angeles, California.
Contact
Dr Saro Armenian
City of Hope
Population Sciences, Outcomes Research
1500 East Duarte Road,
Duarte
CA, 91010
USA
E: [email protected]
T: +1 626 218 7320 Ext. 87320
W: www.cityofhope.org/people/armenian-saro
Creative Commons Licence
(CC BY-NC-ND 4.0) This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. Creative Commons License
What does this mean?
Share: You can copy and redistribute the material in any medium or format







