- Dr Dobri Kiprov, founder and president of Global Apheresis Inc, USA, has been leveraging the power of therapeutic plasmapheresis in treating age-related disorders.
- Plasmapheresis is often used at the far end of the treatment regimen in cases where no other medication has shown any effect.
- Kiprov is researching the different immunoregulatory properties of plasmapheresis and its benefits as a therapeutic and prophylactic measure against neurodegenerative conditions and age-related diseases.
Therapeutic plasma exchange (TPE) purifies a patient’s plasma from toxins. During autoimmune, neurodegenerative, and certain infectious diseases, the patient’s blood becomes infected with toxins and inflammatory markers, contributing to the disease’s severity. Plasma from these patients’ blood containing disease-specific proteins is discarded, and the red blood cells are infused with fresh plasma, albumin (the most abundant protein present in plasma), or a mix of both. The new solution is then re-inserted into the patient’s system.

Past studies have shown that TPE is a safe alternative to intravenous immunoglobulins (IVIGs) – a set of antibodies used to target disease-specific antigens. It can safely discard circulating autoimmune antibody complexes and has immense potential for treating infectious disease-triggered autoimmune conditions. TPE finds applications across 80 diseases to date. It is one of the four major apheresis processes used in medicine, with the other three being erythrocytapheresis (for red blood cells), leukocytapheresis (for white blood cells), and thrombocytapheresis (for platelets).
Unfortunately, in most cases, TPE is the last resort. It’s often used when intensive care patients need to be treated for autoimmune disorders and every other treatment modality has failed. Dr Dobri Kiprov, founder and president of Global Apheresis, Inc, USA, aims to establish TPE as a prophylactic measure, not only for treating immunological disorders but also many neurological, age-related, and infectious diseases.
TPE and ageing
Ageing is a universal process which progressively makes the body susceptible to multiple chronic inflammatory and neurodegenerative diseases. Research has shown that inflammation biomarkers are predictors of morbidity and mortality among older adults. Moreover, animal studies have indicated that heterochronic blood sharing (a process by which an old and young animal of the same species are surgically tied and their circulatory systems are allowed to mix, to study the effects of different circulatory elements in ageing and tissue regeneration) leads to multi-tissue rejuvenation. This strengthened claims that diluting old blood (plasma) in older people can remove pro-geronic factors, rejuvenate old organs, and improve the quality of plasma to support cell proliferation.

TPE is now believed to be beneficial in reversing the ageing process and reviving the cellular and immune complexes which would otherwise stop growing and proliferating. It does so by removing pro-inflammatory proteins and promoting the development of a set of younger circulating proteins in the system of an individual. Kiprov and colleagues showed that TPE could infuse cell-death regulators, regenerative, and anticancer cells, and ensure a younger cellular profile in lymphoid markers, thereby reducing cellular senescence and lowering age-related DNA damage.
Therapeutic plasma exchange can safely discard circulating autoimmune antibody complexes and has immense potential for treating infectious disease-triggered autoimmune conditions.
Kiprov’s work suggests that using 5% albumin as a solution to replace plasma from older individuals can provide meaningful insights into how plasmapheresis can reverse ageing and age-related complications.
Kiprov and colleagues recently completed a placebo-controlled clinical trial confirming his preliminary results.
TPE in neurology: what does the research say?
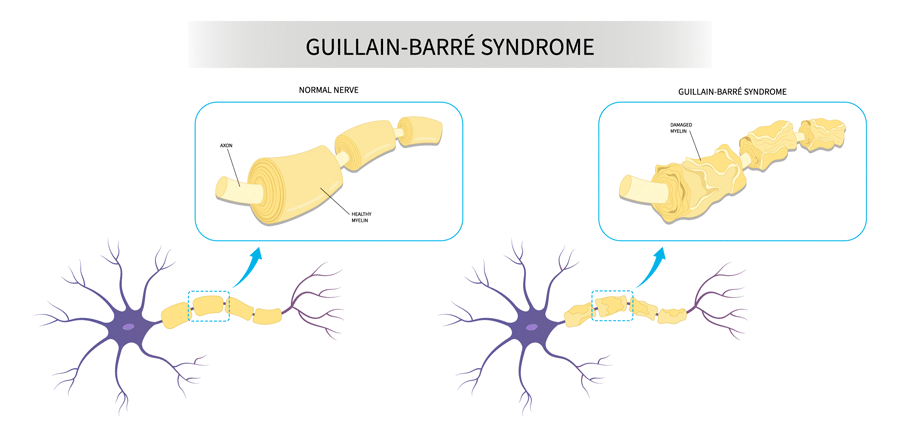
TPE can treat neurological conditions like Guillain-Barré Syndrome (GBS) and chronic inflammatory demyelinating polyneuropathy, and has shown promising results to treat Alzheimer’s disease (AD).
Most people living with AD have plasma containing amyloid beta (Aβ) protein bound to circulating albumin as well as highly oxidised, cysteinylated, and glycated albumin, which impairs albumin antioxidant action. Albumin is the primary antioxidant in the body, so if its function is impaired, this can lead to a build-up of oxidative stress in the brain. This causes excess free radicals to deposit in the brain, resulting in a disrupted nervous system (neurotoxicity). Further, the amount of glycated albumin is significantly higher in plasma than in the cerebrospinal fluid (CSF), making plasma purification a critical step in treating patients with AD. Moreover, previous studies have shown that high levels of plasma Aβ also reduced Aβ clearance from the brain.

Kiprov hypothesises that routine TPE-based removal of the plasma from a person with AD, containing toxic levels of albumin-bound Aβ, might make enough free albumin available to drain Aβ into the CSF. This would result in reduced levels of Aβ in plasma and higher levels in CSF, to be drained out through perivascular spaces around the blood vessels in the brain and the glymphatic system (a drainage system typical to the CNS), among others.
Kiprov and colleagues conducted the Alzheimer Management by Albumin Replacement (AMBAR) trial, a phase 2b/3, randomised, controlled clinical trial. 347 mild-to-moderate AD patients were treated with different replacement doses of albumin, with or without IVIG, to correct a possible immunological deficit. The AMBAR trial effectively demonstrated TPE’s potential to reduce neurodegeneration. 61% of patients with moderately severe AD had their disease progression arrested, while those with mild AD showed significant neurophysiological and neuropsychiatric improvement with a better quality of life. The adverse reactions were mild and noted among 11% of patients.

TPE in long COVID and other infectious disease-triggered autoimmune conditions
The researchers also evaluated TPE’s efficacy in patients with neurodegenerative symptoms secondary to infectious diseases. They examined 17 patients who underwent plasmapheresis at 1–24 months after acute COVID-19 infection (long COVID).
TPE can reduce the number of pro-inflammatory proteins and autoantibodies and create an environment where stem cells and other cells can proliferate.
10 had some form of neuropathy and showed neurotransmitter antibodies on examination, and all reported fatigue, brain fog, anxiety, and depression. TPE showed positive effects on 11 of the 17 patients (~65%): there was a significant reduction in levels of neuropathy, fatigue, brain fog, and risks of coagulopathy. However, anxiety and depression persisted, albeit diminished.
TPE also efficiently treats paediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS). TPE not only proved effective against the autoantibodies produced, but also reduced the neuropsychiatric behaviour among patients which would not subside even after administration of corticosteroids, antibiotics, and high-dose IVIGs.
This included improvements in bladder control, completely subsided suicidal thoughts, improved functional behaviour with peers and family, and better sleep, among others, within 6–12 months of therapy.
The potential of TPE
Kiprov’s research sheds light on TPE’s immunoregulatory effects. TPE can reduce the number of pro-inflammatory proteins and autoantibodies and create an environment where stem cells and other cells can proliferate.
These findings highlight the increasing potential of TPE to be used as a prophylactic and/or immunomodulatory treatment modality for infectious, neurodegenerative, and age-related disorders, with or without pharmacological intervention.

What inspired you to conduct this study?
I knew the scientific and medical potential to expand the use of TPE and tried to clinically prove it.
Can TPE or any form of apheresis-related process completely replace the use of pharmacological intervention, including the administration of antibiotics in infectious diseases?
No, but it can be a very effective complimentary therapy and, in some cases, a complete alternative.
Can TPE be used to treat any genetic or chromosomal disorders?
Cytapheresis provides the cells necessary for genetic and chromosomal manipulation.
Are there any studies on cancer patients to show the effects of TPE on oncology or immunomodulation in oncology?
Cytapheresis plays a vital role in immunotherapy by providing immunocompetent cells.
Is there any evidence for the use of TPE in patients with cardiovascular diseases?
Yes. A special procedure called LDL apheresis plays a role in cardiovascular diseases.









