- Type 2 diabetes and obesity could affect over 700 million people worldwide by 2045.
- Metformin is an effective, widely used diabetes medicine, although its functioning has remained a puzzling mystery until now.
- Professor Jianzhong Shen at Auburn University, USA and his team have uncovered the correlation between metformin controlling higher-than-normal blood glucose levels and the secretion of adenosine triphosphate (ATP) molecules.
- Shen and his team’s continued work could be used to develop novel drug targets for type 2 diabetes.
Obesity and type 2 diabetes are two of the most chronic and prevalent diseases in the USA, estimated to affect 700 million people by 2045. These conditions place a significant financial burden on healthcare systems, with the estimated cost of diabetes in the USA at over $400 billion a year. Type 2 diabetes affects blood glucose regulation, resulting in high blood glucose levels that lead to nervous system, circulation, and immune system damage.

Insulin is released by the pancreas to help liver, fat, and skeletal muscle cells absorb glucose, thus lowering blood glucose. However, both low blood insulin levels and insulin resistance in cells are characteristics of type 2 diabetes. Higher-than-normal blood glucose levels also promote the release of adenosine triphosphate (ATP), an energy-carrying molecule found in cells like liver hepatocytes (cells responsible for metabolism, detoxification, and immune cell activation). People with diabetes usually have high ATP levels in their blood.
An ancient diabetes medicine
Galega officinalis (or galega) plants are rich in the organic compound guanidine and are traditionally used in European herbal medicine to treat diabetes. From 1918, various guanidine-derived diabetes medicines were developed, but eventually discontinued due to toxicity and the increased availability of pharmaceutical insulin.
Metformin is currently the most-prescribed medicine for lowering blood glucose levels, used by over 150 million patients worldwide.
Metformin, a less potent guanidine-derived medicine synthesised in 1922, followed a slower path to diabetes treatment. It was initially employed in influenza cases. In 1957, it was used to address insulin resistance and adult-onset high blood glucose levels. After its adoption in American diabetes care in the 1990s, the long-term cardiovascular benefits of metformin were also identified, further strengthening the argument for its usage. Metformin is currently the most-prescribed medicine for lowering blood glucose levels, used by over 150 million patients worldwide.
Mystery surrounding metformin
Although metformin is extremely effective, the question of exactly how it works is steeped in controversy. Various mechanisms have been suggested, including interactions with gut microorganisms, anti-inflammatory and immunomodulatory effects, and slight inhibition of systems involved in glucose and ATP production inside the cells. Metformin was also thought to stimulate particular liver-cell molecules that activate glucose and fatty acid uptake, although it has the same antidiabetic effect in the absence of these molecules. Almost all previous studies have involved metformin doses 10–100 times higher than therapeutic concentrations, which makes it difficult to understand its action in a clinical setting.

Professor Jianzhong Shen, Full Professor at Auburn University, USA, has focused his efforts on uncovering metformin’s precise mechanism of action. He noted the high ATP levels of diabetes patients, the promotion of ATP release from liver hepatocytes at higher-than-normal glucose levels, and that while metformin reduces glucose levels in diabetics, it tends not to affect these levels in healthy people. Shen and his team aimed to combine these facts to develop a brand new hypothesis describing the way metformin controls higher-than-normal blood glucose levels.
Signalling between cells
P2Y receptors are biomolecules located at the cell membranes that are involved in a process known as purinergic signalling, which allows cells to communicate and carry out their functions. These receptors are stimulated by molecules such as ATP and play an essential role in liver function. Certain P2Y receptors have been linked to metabolic diseases (disorders that negatively affect the way the body handles proteins, fats, and carbohydrates).
Shen and his team first considered whether metformin could directly block P2Y receptor activity. The team demonstrated that high blood glucose levels triggered ATP release from human skeletal muscle cells, and that this ATP activated a particular P2Y receptor (P2Y2R), compromising insulin signalling and leading to insulin resistance.
Visualising ATP secretion
Although the team obtained groundbreaking results on skeletal muscle cells, they could not confirm whether metformin had a direct effect on P2Y2R activity when studying another cell type, liver hepatocytes. This led Shen and his team to explore whether metformin might indirectly affect P2Y receptor signalling by blocking ATP secretion.
The team successfully observed this indirect effect and designed various experiments to better understand the underlying mechanisms. They demonstrated that high blood glucose promotes ATP release from hepatocytes, and that through P2Y2R signalling, this ATP triggers the release of more glucose from the liver into the blood.

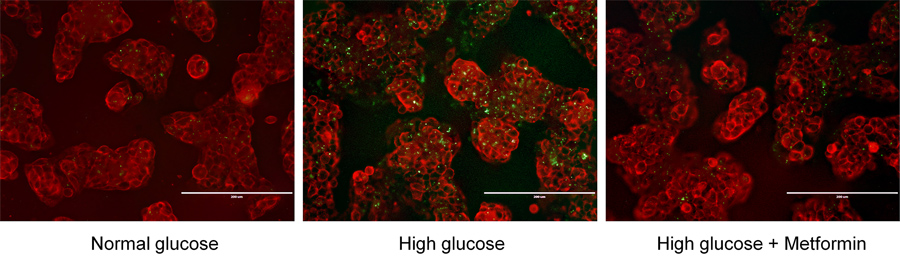
The team visualised ATP secretion during a groundbreaking experiment in which they forced hepatocytes to express a type of molecular ATP sensor. The sensor emitted a green-fluorescent light when binding to extracellular ATP at doses over 10µM, which was suppressed by 10µM metformin, allowing the team to confirm that metformin treatment dramatically inhibited ATP release.
Insulin resistance in mice
Shen and his colleagues studied mice with and without the gene required to produce P2Y2R. The team discovered that a low metformin dose of 10µM completely blocked ATP secretion in response to high glucose levels in both laboratory cell cultures and mice. They also found that metformin significantly improved insulin tolerance in mice on a high-fat diet, and that it only worked in mice with the P2Y2R gene and high blood glucose.
Shen proposed that glucose-stimulated ATP secretion is the mechanism by which insulin-sensitive tissues (cells that use blood glucose effectively to reduce blood sugar) control glucose regulation through AKT signalling, a process that promotes glucose use and molecule synthesis in fat tissues. The team confirmed that ATP utilises P2Y2R receptors to inhibit insulin-induced AKT signalling, while also promoting glucose production in the liver, leading to high blood glucose levels. The results of the experiment are in accordance with recent research indicating that various P2Y receptors promote high-fat diet-induced obesity and insulin resistance in mice.
Unravelling metformin’s functionality
Shen and his team demonstrated for the first time that metformin limits ATP release from cells, thereby reducing ATP-activated purinergic receptor signalling and controlling higher-than-normal blood glucose levels. Shen explains that the next step in understanding metformin will be to determine exactly how it suppresses ATP secretion in response to high glucose levels, and the team has significantly narrowed the field of investigation down to a disruption of ATP release.
The team demonstrated for the first time that metformin limits ATP release from cells, thereby reducing ATP-activated purinergic receptor signalling and controlling higher-than-normal blood glucose levels.
Shen and his team’s landmark research shines a light on how metformin could possibly work, with a view to exploring other novel drug targets in the continuing battle against diabetes and obesity.
What spurred you to investigate the mechanism behind metformin – a drug that has been in use for 70 years?
In 2014, my mom suffered a car accident, and when she was brought to the hospital, the doctor told us that she had very high blood glucose levels. It was determined that she had type 2 diabetes after further diagnosis. The physician prescribed metformin for my mom, and she has had good control of her blood glucose levels after taking metformin for just a few weeks. It was then that I started to look at a pharmacology textbook to see how metformin works for type 2 diabetes. To my surprise, there was no clear description of the molecular mechanism of action for metformin in several well-known pharmacology textbooks. This intrigued me very much as a pharmacology professor, especially considering that metformin has been used in the clinic for so many years. Coincidently, at that time, I had a new graduate student whose dad was diagnosed with type 2 diabetes as well and started to take metformin. We then decided to study how metformin works in human skeletal muscle cells to control the interaction between insulin and purinergic signalling towards glucose uptake.
On the other hand, the pharmacology history told me that studying the exact mechanism for an effective clinical drug with unknown mechanisms could be very rewarding. For example, nitroglycerin has been used to relieve chest pain (angina) in people who have heart attacks for almost one century and saved countless people’s lives; however, its mechanism of action was not known until the early 1980s when a pharmacologist, Dr Loius Ignarro, demonstrated that nitroglycerin releases a gas molecule called NO (nitric oxide) to dilate the coronary arteries, a discovery leading to the 1998 Nobel Prize in physiology and medicine.
What could the clinical impact of this improved understanding of metformin’s mechanism of action be?
This improved understanding of metformin’s mechanism of action may not change the clinical practice of metformin use for treating diabetes. However, it does imply that we may be able to develop more specific new drugs to block the P2Y2 purinergic receptor to achieve the same or better clinical efficacy in treating type 2 diabetes, but bearing much fewer side effects than metformin does. Please note that gastrointestinal intolerance to metformin remains a problem for many diabetic patients, and some diabetic patients are just not sensitive to metformin for unknown reasons.
Could your findings on glucose control mechanisms be applied to treating other medical conditions?
Historically, it was thought that our body’s cells control glucose uptake based on the level of ATP inside the cells. Our finding indicates that when our cells have enough ATP inside, some parts of the ATP pools can be released outside the cells to slow down glucose uptake through purinergic control of insulin signalling. However, such a fine-tuning mechanism was over-activated in disease states like diabetes due to P2Y2 receptor upregulation or excessive ATP accumulation outside the cell membranes. It is clear now that metformin can tape down the purinergic signalling in diabetes, but we believe such a negative control mechanism for metformin could be responsible for many, if not all, clinically observed benefits for metformin-takers, including anti-cancer, anti-inflammatory, anti-ageing, and even anti-COVID-19 effects.
How significant is the link between obesity and diabetes?
The link between obesity and diabetes is substantial. Obesity is a major risk factor for type 2 diabetes, as excess body fat, especially around the abdomen, can lead to insulin resistance, where the body’s cells don’t respond appropriately to insulin. Over time, this can result in high blood glucose levels and the development of type 2 diabetes. Interestingly, we published a new paper recently to show that overfat boosts the ATP purinergic signalling in adipocytes, a type of fat cells. Thus, maintaining a healthy weight through diet and exercise is crucial in preventing and managing diabetes.
What is next for you and your research team?
Well, lots of important questions remain. We are in the process of revealing how many tissues or organs’ P2Y2 receptor signalling can be impacted by metformin. We believe liver hepatocytes are not the only cells affected by metformin. In addition, as mentioned above, we are also hoping to validate if some of the pleiotropic effects of metformin are due to its suppressive action on ATP release. Of course, the most challenging question is how exactly metformin blocks cellular ATP release in response to higher-than-normal glucose outside the cells. I wish more scientists would be interested in this new direction so we can someday update the textbook and improve patient care.