The primary function of the human respiratory system is to breathe in oxygen and excrete carbon dioxide. Oxygen passes from inhaled air in the lungs into the circulatory system. In contrast, carbon dioxide passes from the blood into the cells and alveoli in the lungs and is then exhaled. The goal is to have enough oxygen and maintain normal levels of carbon dioxide in the body; the latter is just as important as the former.
Special receptors called chemoreceptors are primarily able to sense CO2 (carbon dioxide) and pH, and only secondly oxygen levels. When these parameters change, the counter-regulation implements changes which aim to restore the normal levels – sometimes it conflicts with unsolvable contradictions, if all three cannot be met.
Hypocapnia (a reduced carbon dioxide level in the blood) is usually caused by deep or rapid breathing (hyperventilation). It is often associated with high arousal states including anxiety and panic disorder; anxiety can be the cause or a consequence of the hypocapnia, possibly both.
Hypocapnia can alkalise both the blood serum and the inside of the body’s cells. This can have rather significant effects on other molecules in the blood and cells, such as calcium ions which are essential for nerve and muscle excitability. Consequently, the symptoms of low levels of carbon dioxide may include tingling limbs, disrupted heart rate, muscle cramps, seizures and many more.
Opposed to this, hypercapnia is the occurrent of increased levels of carbon dioxide in the blood, often secondary to decreased breathing rate, lung disease or a state of reduced consciousness.
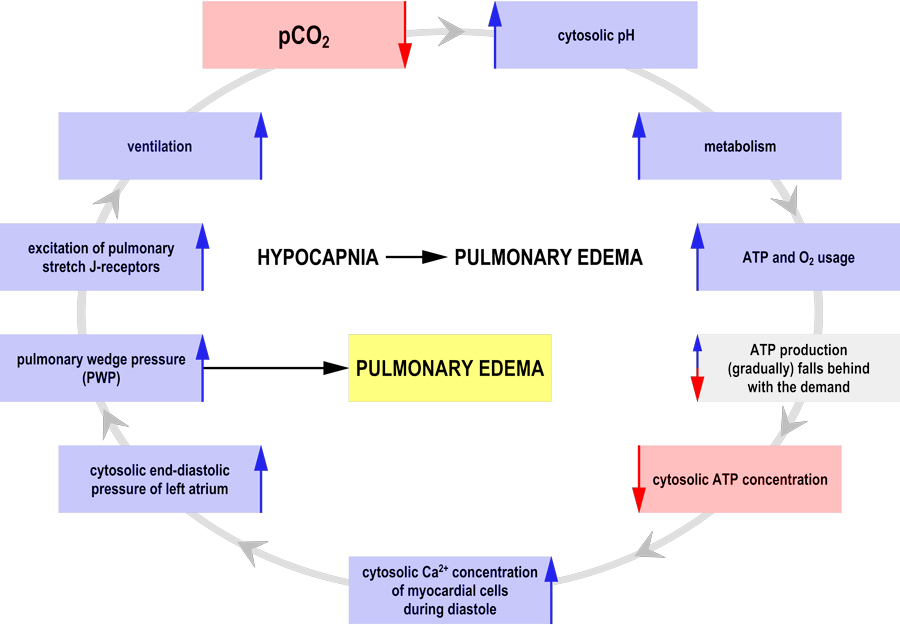
Dr András Sikter works alongside the Municipal Clinic of Szentendre, Hungary, to explore how changes in hydrogen ion concentration (pH) due to hypo- and hypercapnia impact upon cell metabolism and how they can induce diseases of civilisation. In this work he has explored those vicious circles in which hypocapnia on its own can accelerate metabolism through intracellular alkalosis and ultimately lead to fatal outcomes. If his hypothesis is true, the therapeutic strategy of emergency medicine should be modified because hypocapnia often leads to death in critically ill patients for example, due to congestive heart failure, lung diseases, high altitude sickness, stroke, brain trauma, meningitis, sepsis, COVID-19 infection, etc.

Changes in acidity levels
Any change in carbon dioxide levels, and therefore respiration, will affect the pH of cells. It takes hours or days for the compensatory mechanisms to kick in, by which time fatal damage could have already occurred in the case of hypocapnic emergency. The compensatory processes are also not complete and optimal as the numerous counter-regulation mechanisms appear to contradict even each other or create additional errors secondary to trying to restore intracellular pH; this is the case in chronic ventilatory disorders.
The regulation of intracellular H+ concentration (pH) has priority above other ions, often at the expense of them.
Intracellular pH has a number of very significant impacts on the rates of metabolic reactions and energy demand. Due to this, if it differs from the normal levels, the regulation of intracellular H+ concentration (pH) has priority above other ions, often at the expense of them.
Generally, alkalosis (increased pH) causes cell metabolism to increase, whereas acidosis (decreased pH) slows it down. As a result, energy demand also increases or decreases. A small increase in pH results in a huge increase in cell metabolism and excitability of neurons, muscles cells and cardiac cells. Cell excitability is defined as cells being activated by, and reacting to, a stimulus such as an electrical signal. It is often induced by changes in the cell membrane potential, i.e. the differences in the concentrations of ions on opposite sides of the cell membrane. During steady-state, the ratio of these ions remains unchanged.
Energy demand and production
Adenosine triphosphate (ATP) is the energy currency of a cell and plays a key role in metabolism. Hypocapnia increases cells’ oxygen and ATP energy utilisation. Young, healthy tissues are able to adjust their ATP production to meet increased demands. However, the cell membranes can become more permeable to other molecules, such as calcium ions, which can lead to excitability problems and symptoms of functional disorders.
Dr Sikter explains that in contrast, seriously damaged tissues are unable to meet this demand; for example, the heart tissue may be impaired due to another illness/disease. In these cases, the attempt to meet energy demands, and the subsequent failure to provide an adequate amount of ATP, can lead to a series of further complications such as fluid accumulation in the lungs. Dr Sikter highlights that low phosphate levels in the blood can also arise from hyperventilation, resulting in further ATP deficiency and exacerbating the whole issue.

Permissive hypercapnia
Critically ill hypocapnic patients suffering from ARDS or COVID-19 infection undergoing mechanical ventilation are often placed in the state of ‘permissive hypercapnia’ by physicians. A controlled high carbon dioxide level has a therapeutic effect on infected lungs and is not life-threatening if sufficient oxygen is available at the same time. Because the developing acidosis has the ability to slow down metabolic and enzymatic processes, this can potentially be lifesaving in the short term. The ‘permissive hypercapnia’ theory and practice, formed by experience of the pioneer physicians, is now generally accepted by the medical community and researchers after twenty years of struggle. Nevertheless, there is no other means in our hands to safely alter CO2 levels as the mechanical ventilation.
In contrast, acute hypocapnia can further endanger critically ill cells or organs due to the increased energy demands which they are unable to meet. Hypocapnia has an immediate impact on cell metabolism, whereas counter-regulation takes longer to respond. This means that each cell is left to meet increased energy demand alone before compensatory mechanisms kick in. This is achievable for young, healthy tissues but not for those who are seriously damaged or impaired (‘the weakest link’).
This correlation is also seen when heart function is considered; heart failure increases oxygen demand as the damaged tissues have to work harder to match the work of a normal heart. The development of hypocapnia during congestive heart function is a marker for poor prognosis as it reflects the exhaustion of the heart’s energy reserves and hypocapnia demands a further increase in ATP. It was found by others that low-dose carbon dioxide treatment could theoretically reduce the risk of hypocapnia generated by congestive heart failure. However, Dr Sikter notes that this needs further research.
Dr Sikter concludes that ‘the ability to provide energy supplies can be an important dividing line between organic and functional diseases’.
The vicious cycles of mental and somatic illnesses
The link between mental and physical health is well known. For example, people will increase or decrease their breathing rate in line with emotions and arousal, thus inducing hypo- or hypercapnia. Dr Sikter identified that vicious cycles will develop involving somatic and functional changes; they almost inevitably develop in the case of hypocapnic emergency. However, there is a narrow path (such as ‘permissive hypercapnia’) to recovery. The occurring acidosis is able to break the vicious circle and turn it into a virtuous cycle.
Delirium is common when cells of the brain have been damaged, and symptoms can include hyperventilation. This could also go some way to explain the link between hyperventilation, anxiety and longer-term damage; hyperventilation may kill or damage the injured brain cells further, suggesting an explanation for the progression of underlying diseases during delirium.
Hyperventilation hypocapnia in individuals with panic disorder can result in cardiac arrhythmias and, while panic disorder does not cause coronary artery disease, it can double the chance of death if the two disorders occur at the same time.

Dr Sikter’s earlier work has also explored the relationship between physical and mental health. He suggests that protracted or repeated episodes of major depression could lead to actual physical damage to the brain and other critically ill organs. That is why Major Depression is more of an organic rather than a functional disorder – according to Dr Sikter’s theory, chronic (respiratory or metabolic) acidosis promotes its development. He concludes that ‘the ability to provide energy supplies can be an important dividing line between organic and functional diseases.’ To expand on this, organic diseases involve an observable and measurable disease process, such as inflammation, whereas functional diseases have no definite somatic direction to explain disease occurrence.
Although generally thought not to be dangerous, Dr Sikter discusses that hypocapnia can have fatal results for those who are critically ill, and the deciding factor appears to be whether the cells are able to mobilise sufficient ATP to meet increased energy demands. He believes that administering physiological doses of certain (to be tested) natural salt-mixtures could normalise elevated or decreased carbon dioxide levels, and thus recover intracellular ion status and normal metabolism.
And there is something else: chronic hypo- and hypercapnia both lead to serious regulatory and balance problems, for which we currently have no solution. But the situation is much more serious now when we don’t even notice those problems.
more consideration in the pathophysiology of human diseases?
We must not tolerate the persistence of higher or lower carbon dioxide levels. In the long run, the compensation promotes only the survival of respiratory disorders, which can be important stages in the development of the diseases of civilisation. We have to work out a widely applicable strategy to restore CO2 levels to normal. As we demonstrated, even hyperventilation alone can be fatal in critically ill patients (‘permissive hypercapnia’ can also be used only in the short term). All cells have to fight alone against the intracellular alkalosis caused by hypocapnia, the critical ATP deficiency will develop in the Paths of Least Resistance.
References
- Sikter, A. (2018). Hypocapnia and mental stress can trigger vicious circles in critically ill patients due to energy imbalance: a hypothesis presented through cardiogenic pulmonary oedema. Neuropsychopharmacologia Hungarica, 20(2), 65–74. Available at: https://pubmed.ncbi.nlm.nih.gov/30131453/
Research Objectives
Dr Sikter investigates ATP production and use during acute hypocapnia.
Bio
Dr András Sikter is an internist and cardiologist. From 1973, he worked at St. Rokus Hospital in Budapest where even physician Semmelweis once practised. Since 2007, Sikter is at the Municipal Clinic of Szentendre. During his decades of work, he has developed a simple cytoplasmic model that has proven to explain the mechanisms of many organic and functional diseases as well as providing their recovery strategy.
Acknowledgements
I thank Prof Zoltán Rihmer and Prof Gábor Faludi, psychiatrists that were very supportive of my work and the appearances of my articles in Neuropsychopharmacologia Hungarica.

Contact
Dr András Sikter
SZEI (Municipal Clinic of Szentendre)
Kanonok u. 1.
Szentendre
H-2000
Hungary
![]()
E: andrassikter3@gmail.com
E: sikter.andras@szeirendelo.hu
T: +36 26 393129