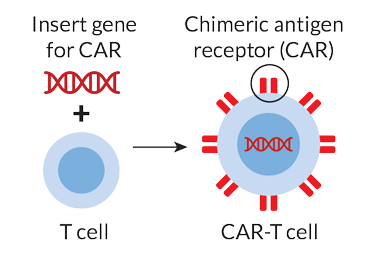
Identifying CAR-T cells
Chimeric antigen receptor T cells (CAR-T cells) are T cells that have been genetically modified to produce an artificial T cell receptor. This T cell receptor can then be used in immunotherapy. Chimeric antigen receptors (CARs), also known as chimeric immune-receptors, chimeric T cell receptors, or artificial T cell receptors, are receptor proteins created to give T cells the capacity to target a specific cellular markers. The receptors are presumed to be chimeric because they integrate antigen-binding and T cell activation activities into a single receptor.
The rationale behind CAR-T cell therapy
CAR-T cell immunotherapeutic treatment is a technique based on the optimisation of the human body’s immune system so that it becomes better adopted to identify and eliminate cancer cells. T cells are considered as the first line of the body’s natural defence mechanism against cancer, and the human immune system is naturally prepared to fight off the tumour cells. CAR-T cell treatment, which can be either autologous (from the patient) or allogeneic (from a donor individual of the same species), fundamentally improves the function of T cells.
In autologous CAR-T cell mediated immunotherapy, medical practitioners will determine the particular antigen generated by the specific malignancy that the patient is dealing with. They create T cells to express a CAR on their surface membrane so that it will detect and bind that particular antigen once they have extracted T cells from the patients. The patient is then re-infused with this altered population of cells, which acts as a “living medicine” or “alive medicine” that may detect and eliminate malignant or tumour cells in the blood. Before being infused into the patient, the cells utilised in allogeneic CAR-T are taken from a healthy donor and modified to express the precise needed CAR.
Perceptions of CAR-T cell therapy in oncology
Traditional or conventional cancer therapies like chemotherapy and radiation therapy are unable to distinguish between malignant and healthy cells. This indicates that both types of cells are destroyed during therapy, resulting in undesirable side effects and ‘collateral damage’ of normal tissue. CAR-T treatment, in contrast, combats cancer by harnessing the patient’s own immune system. This could represent an illustration of the so-called ‘personalised medicine’ or ‘precision medicine’, in which a patient’s therapy is adapted to their specific needs, in light of their illness and genetic makeup. Because CAR-T is a targeted therapy, only cancer cells (and not healthy cells) will be eliminated, resulting in fewer adverse effects. The cells also reproduce and continue to target cancer cells after being transfused back into the patient’s circulation, making it a resilient and durable alternative without the need for repeated or continuing therapies.
Insights gained from using CRISPR for CAR-T cell therapies
The efficacy and safety of CAR-T cell treatments can both be increased by the use of CRISPR gene editing. When taken in comparison to previously used editing technologies, CRISPR is considerably more accurate in terms of engineering genomes. As a result, CRISPR is less harmful to patients as it is able to target more closely. It can also produce several gene alterations in T cells, which has previously been a difficult task. The precise insertion of the CAR into the appropriate location in the T cells’ genome so that it is produced at a sufficient level is one method CRISPR may be employed. Additionally, it can be utilised to fix genetic flaws on autologous T cells, some of which prevent the cells from properly locating and eliminating cancer cells. CRISPR modifications can also improve CAR-T cells’ capacity to attack cancer cells.
The capability of CRISPR to produce universal or ‘off-the-shelf’ CAR-T cells makes it a crucial tool in CAR-T treatment. With the idea of universal allogeneic CAR-T products, there is no longer a need to collect, modify, grow, and transfuse T cells from each unique patient, which saves time and money.
Allogeneic (healthy donor) T cells can be safely transfused into patients without running the danger of immunological rejection by first being edited to express the CAR by knock-in and then having the genes that the immune system uses to recognize these non-self-cells knocked off. These CRISPR-edited designer cells may be mass-produced, cryopreserved, and kept at hospitals or other facilities across the nation, doing away with the need to move living cells between manufacturing sites and hospitals for every patient.