
- An increasing prevalence of fatty liver – called steatosis – is exacerbating the global shortage of acceptable livers for transplant.
- Dr Carmen Peralta’s group at the Hospital Clínic de Barcelona, Spain, researches ways of protecting livers from pathologies during transplantations and resections to improve survival odds.
- Their recent work reveals that steatosis status determines inflammation and molecular signalling pathways.
- Understanding these pathways may enable the development of therapies and strategies to improve the success of liver transplants.
- This novel study provides a solid foundation to incorporate these laboratory findings into clinical practice.
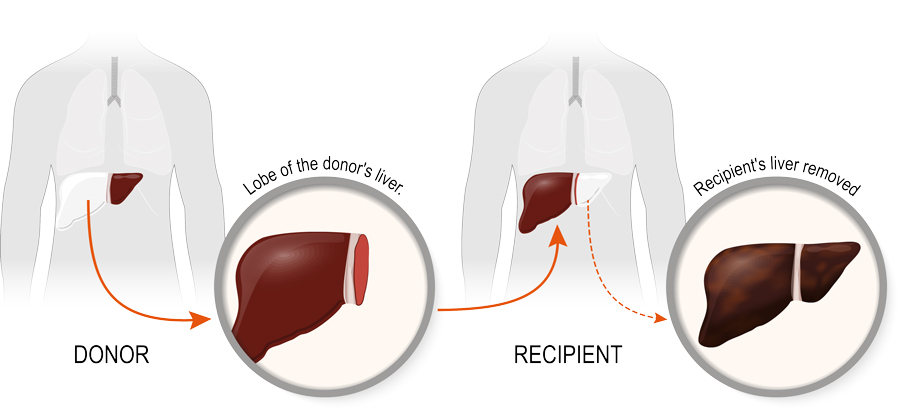
For patients with end-stage liver disease, a liver transplant is often the best and only treatment option. This major operation carries risks but, if successful, helps them live longer with a better quality of life. Unfortunately, too many people die waiting for a liver transplant due to global donor shortages. Most liver donations are from brain-dead individuals or other cadaveric donors, both inherent risk factors threatening a successful transplantation. Additionally, up to half of donor livers have fat build-up in their cells, a condition known as steatosis, which can cause liver dysfunction and, further, decrease transplant survival rates.
Declining steatotic livers for transplantation exacerbates the global donor shortage.
Declining steatotic livers for transplantation exacerbates the global donor shortage. One way to address this issue is to reduce the risks of liver dysfunction in steatotic livers donated by brain-dead donors. To do so, we first need to understand the inflammation and damage associated with steatotic livers from brain-dead donors to develop therapies.

In their groundbreaking paper published in Frontiers of Immunology, Dr Carmen Peralta’s group at the Hospital Clínic de Barcelona, Spain, makes vital inroads to address this need. They discovered inflammatory and signalling pathways in both steatotic and non-steatotic rat livers to expose therapeutic targets, in the hope of improving post-transplant outcomes.
Cryptic codes
The research team conducted a series of experiments in brain-dead rats with the aim of unravelling the molecular signalling mechanisms in liver transplants from both steatotic and non-steatotic livers. Cytokine proteins are chemical messengers that coordinate essential physiological processes and immune responses. They can be both pro-inflammatory and anti-inflammatory, and their dysfunction is implicated in disease.
A group of cytokines called interleukins regulate inflammatory and immune system responses. Two of these, namely IL-6 and IL-10, are known to protect the liver against ischaemia-reperfusion (I/R) injury. This type of injury occurs during liver surgery and can cause liver dysfunction post-transplant. I/R injury occurs because reduced blood flow to the liver induces hypoxia (low levels of oxygen) and kills cells, a condition that paradoxically worsens when blood flow is restored.
In a first-of-its-kind study, Peralta and colleagues used blood and tissue samples from both steatotic and non-steatotic livers to investigate the role of these two cytokines in liver transplantation from brain-dead donors. Suspecting a potential regulatory mechanism, they studied these two cytokines and the pro-inflammatory cytokine IL-1β, as well as the role of nitric oxide (NO). Nitric oxide has been shown to regulate cytokines, in particular IL-1β, and in doing so reduces its inflammatory effects and induced damage. The team wanted to explore the role of NO further and determine if it also regulates other interleukins during liver transplant.

Points of difference
The effects of brain death on cytokine messaging are different in steatotic compared to non-steatotic livers. For example, brain death diminishes the protective effects of IL-10 in steatotic livers and IL-6 in non-steatotic livers. However, the downstream effect of both is an increase in IL-1β, which, in turn, enhances inflammation and damage. To counteract this, the researchers treated steatotic rats with IL-10 and those with non-steatotic livers with IL-6. This actively reduced IL-1β induced inflammation and damage. By demonstrating this, the team opened therapeutic avenues to reduce the pathology seen during liver transplantation.
Because there is no easy and immediate way of knowing if a liver from a donor is steatotic or not, the researchers propose using only therapies appropriate for both conditions.
If NO is blocked, IL-10 and IL-6 are further depleted in steatotic and non-steaotic livers, respectively. This has the knock-on effect of further increasing IL-1β levels and its destructive inflammatory effects. As the researchers expected, administering NO to non-steatotic livers improved IL-6 levels, therefore reducing IL-1β and associated inflammation and damage. Surprisingly, the opposite was found in steatotic livers where NO donor treatment did not improve IL-10 and IL-1β levels but instead worsened the damage and inflammation. Understanding and appreciating these specificities will allow researchers to develop therapies suitable to both conditions, ultimately reducing complications following transplant. This study also highlights that the time between the donor being declared brain dead and liver retrieval is a critical period where intervening can help prevent any adverse side effects.
Appreciating the differences in signalling pathways between steatotic and non-steatotic livers during liver transplants from brain-dead donors aids treatment design. Because there is no easy and immediate way of knowing if a liver from a donor is steatotic or not, the researchers propose using only therapies appropriate for both conditions, such as an IL-1β inhibitor. These preclinical experimental findings provide a platform to take this work forward in future research, exploring therapeutics for patient benefit. Establishing clinical relevance in humans would be a major step forward in reducing liver transplantation waiting times.

What led you to study the field of liver transplantation and resection?
Obesity, and thus steatosis, is becoming more common by the day. Moreover, according to national and international organ transplantation societies, more transplants are performed each year. That is why finding new strategies to protect steatotic livers from cadaveric donors – which currently make up about 50% of the grafts, and the rate is increasing – is an urgent clinical need to improve post-operative outcomes and reduce waiting lists. The same happens with liver resections. Ischaemia-reperfusion injury produces regenerative failure that is exacerbated in liver from steatotic individuals. Regeneration is a process that is crucial after liver resection, and due to the increase of obesity and steatosis, protect livers from this damage after resection surgeries is a current clinical need.
What is one common misconception people have about your work?
People tend to think that all organs are suitable for transplantation and that transplantation is always a definitive and efficient treatment. A high percentage of livers from cadaveric donors have to be discarded because of their condition (due to lifestyle, age, steatosis, viral infections, etc). Moreover, liver transplantation is not always the best option. A lot of people who’ve received a transplant need a re-transplantation due to a number of reasons: the graft suffers damage causing liver dysfunction or the recipient lifestyle is not the appropriate after transplantation surgery, among other reasons.
How do you take this work forward from animal models to humans?
First of all, it is important to know if the signal pathways studied by our group are the same in humans. This can be confirmed using biopsies from human samples. Security clinical studies with potential treatments have to be performed in order to discard adverse effects of novel therapies. Another way to translate our preclinical results into clinical practice is to study if the pathways established by our group in preclinical models are the same in discarded organs. If we could study samples of these organs using an ex vivo model and report the same affected pathways, our therapies could be used to avoid discarding these grafts.
The translation of our results to clinical practice is not new to us. Dr Carmen Peralta demonstrated the benefits of ischemic preconditioning in preclinical practice, a surgical technique that was later applied to clinical practice. Moreover, other preclinical studies directed by Dr Peralta have been translated to the clinic and are now being studied in humans as a novel transportation advice for grafts using ultrasounds.









