Peroneal or tibial nerve transfer operation makes strides for treatment of foot drop
Health & Medicine
ArticleDetailDownload PDF
Patients with foot drop find it difficult to lift the front part of their foot and toes. It is a debilitating condition, yet current treatments are limited. Pioneering a new surgical technique involving nerve transfer, Dr Rahul Nath, Director of the Texas Nerve & Paralysis Institute is set to change this. Through the successful treatment of over a hundred patients, Dr Nath shows that this is a feasible and effective management option for foot drop.
‘Foot drop’ is a deceptively simple name for what is often a complex problem. It is a general term describing the loss of ability to raise the foot at the ankle, leading to difficulty in walking and a floppy-appearing foot. There are many causes of foot drop, but one important reason is damage to the nerves controlling the leg muscles that are responsible for bending and lifting the front part of the foot and toes. This causes a person to either drag the foot and toes or, to compensate, use a high-stepping walk called ‘steppage’ gait. This way of walking requires more effort and in time may lead to further problems, such as back or hip pain. Foot drop often causes pain or uncomfortable neurological symptoms, such as tingling or burning. The combination of decreased mobility and pain limits daily activities and has a devastating impact on the patients’ quality of life.
Pioneering the use of a new surgical procedure involving nerve transfer, Dr Nath has successfully treated over a hundred foot drop patients.
Figure 1: The incision at the popliteal fossa.
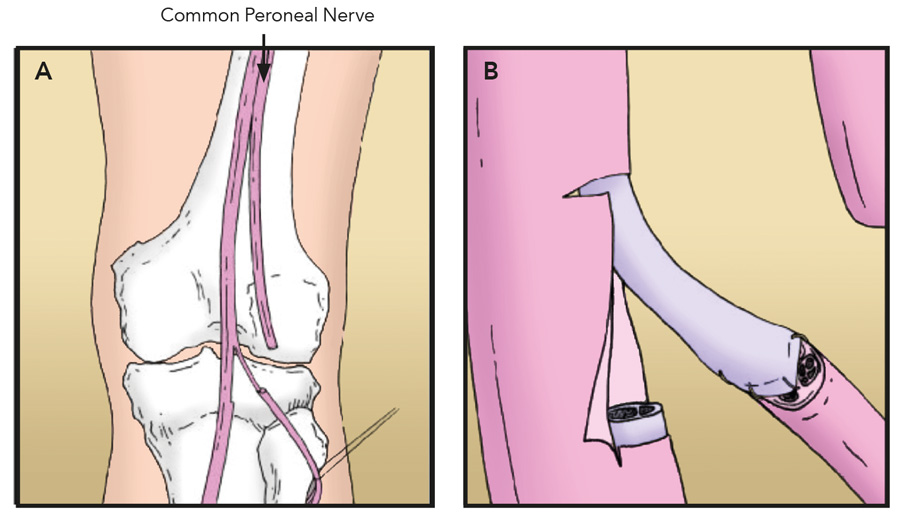
Foot drop is commonly caused by injury to the peroneal nerve. The peroneal nerve wraps from the back of the knee around to the front of the shin, and supplies movement (motor control) and sensation to groups of muscles within the lower leg, foot and toes. As this nerve supplies the tibialis anterior muscle (TAM), which is responsible for lifting the foot, any damage which disrupts the motor control pathway between the peroneal nerve and TAM can result in foot drop. The peroneal nerve is susceptible to damage since it lies very close to the surface of the skin. Consequently, it is commonly compressed or damaged through sports injuries, gunshot wound, hip or knee replacement surgery, childbirth, or diabetes. Pathologies such as multiple sclerosis, stroke, spinal cord injury or cerebral palsy may also cause foot drop. Managing the ups and downs of foot drop
There are limited treatment options for foot drop, and these vary according to the cause and level of nerve injury. A brace (ankle-foot orthosis) can be fitted to help support the foot and improve walking ability, however many users find them uncomfortable and unhygienic. For some, nerve stimulators (which apply small electrical charges to the leg) may help improve mobility. In patients where the nerve does not recover, surgery is then considered. Peroneal nerve decompression is an option for compressed nerves; or surgery to transfer tendons from stronger muscles may improve ankle mobility but provides only a small improvement in gait and ankle movement and comes with the risk of long-term complications. Nerve graft is a limited treatment option, carried out only when a small length of the nerve is affected (less than 6cm). Generally, however, foot drop is difficult to manage successfully. This is where the work of Dr Rahul Nath, Director of the Texas Nerve & Paralysis Institute comes in. Pioneering the use of a new surgical procedure involving nerve transfer, Dr Nath has successfully treated over a hundred foot drop patients.Figure 2: (A) Exposure of the peroneal nerve at the fibular neck after intraneural dissection within the substance of the common peroneal nerve. (B,C) Partial superficial peroneal nerve in the treatment of deep peroneal nerve injury. Two fascicle groups of the superficial nerve suffice to neurotize the deep peroneal distal stump.Figure 3: (A) Exposure of the peroneal nerve at the popliteal fossa. (B) Cross section of common peroneal nerve at the popliteal fossa indicating the topography of the fibers to the tibialis anterior.Cutting edge medicine
Nerve transfers involve taking nerves with less important roles (or branches of a nerve that perform redundant functions to other nerves), and ‘transferring’ them to restore the function of a more crucial damaged nerve. Dr Nath describes it as ‘converting a high-nerve injury to a low-nerve injury.’ This type of surgery has been successfully used to treat upper arm nerve injuries and facial paralysis. Dr Nath is spearheading the technique for damaged deep peroneal nerves – offering relief to patients with foot drop. Covering new ground for foot drop treatment
In a ground-breaking study, Dr Nath treated 14 patients who had suffered foot drop resulting from deep peroneal nerve damage. For each patient, Dr Nath’s first task was to find a suitable donor nerve – a healthy, functioning motor nerve (controlling movement), ideally located as close as possible to the target muscle (the shorter distance over which a nerve has to regenerate, the better the chances that it will reinnervate its new muscle).Ankle dorsiflexion of a patient prior to (A,B) and 14 months following tibial to peroneal nerve transfer (C,D).
Dr Nath found two nerves that could serve as suitable as donors, and careful assessment of nerve function guided the choice of donor nerve. A branch of the peroneal nerve (named ‘superficial peroneal nerve’) was favoured if found to be functional, however, if the injury had affected superficial branches of the peroneal nerve as well as the deep peroneal nerve, then the tibial nerve was selected as donor. Once the suitable donor nerve was found, it was then transferred or ‘plugged in’ to the injured nerve, with the aim of controlling movement of the tibialis anterior muscle.
After surgery, patients did not lose function in their donor muscles. In time and following physiotherapy, the patients were assessed to see whether they had regained function in their TAM after nerve transfer. Dr Nath measured muscle strength of the foot before and several months after surgery. On follow-up, 11 of the 14 patients showed significant improvements in their control of foot movement. The internationally recognised Modified British Medical Research Council Motor Scale (BMRC) was used to assess muscle strength – where zero indicates no movement, and five is normal function. Before surgery, all 14 patients scored zero for ankle dorsiflexion (the movement that brings the toes closer to the knee, as if pulling up off the gas pedal). Following surgery, 11 patients scored between three+ to five, and one patient scored three, showing that their TAM had been successfully innervated by the donor nerve. The two remaining patients had no improvement, possibly because the donor nerves were not as healthy prior to surgery. Dr Nath concluded that only donor nerves with a BMRC score of four or higher should be used, to ensure a good outcome for the patient.Figure 4: (A,B) Partial tibial nerve transfer in the treatment of deep peroneal nerve injury.Making strides
In a second study, Dr Nath carried out the nerve transfer procedure in 21 patients with foot drop due to severe peroneal nerve injury. All patients had no dorsiflexion movement in their ankle (BMRC score 0) due to their injuries, and also scored poorly for eversion movement (flexing the ankle down, as if pushing the gas pedal down). As before, Dr Nath first assessed nerve function, to determine which nerve would be selected as the donor, and either the superficial peroneal nerve or tibial nerve was chosen as appropriate. To optimise the chances of success, Dr Nath precisely measured the correct length of donor nerve to transfer. This ensured that a tension-free link was made between the two end segments of the damaged nerve, since tension can compromise recovery for nerve transfer.
Patient outcomes were assessed between six to 50 months post-surgery. A significant improvement in ankle dorsiflexion and eversion movement was achieved in 80% of patients. Their foot drop had been corrected and they no longer had a steppage gait. In the other 20%, there was good improvement in ankle eversion but not in dorsiflexion. Dr Nath believes that successful treatment is attributed to careful selection of the donor nerve (tested by electrical stimulation) and optimal timing of the operation after injury (injuries of less than one year of duration).
There are limited treatment options for foot drop, and these vary according to the cause and level of nerve injury.
Given the success of Dr Nath’s treatment for foot drop patients, it is no wonder that he has been elected one of America’s Top Doctors for three years in a row, a prestigious award bestowed on less than 1% of American doctors. His new surgical technique gives those with foot drop a feasible and effective treatment option for the debilitating condition, restoring quality of life.
What do you feel are the key factors attributing to a good outcome for patients following tibial or peroneal nerve transfer procedure?
It is known that the experience of the surgeon has an impact on functional recovery and outcome in patients after any surgery, as well as in the repair of nerve injuries. As I have performed thousands of peripheral nerve surgeries and over a hundred foot drop nerve transfer operations, improvements in these foot drop patients are excellent.
References
Nath R, Lyons AB, Paizi M. Successful management of foot drop by nerve transfers to the deep peroneal nerve. J Reconstr Microsurg. 2008; 24:419-427.
Nath RK, Somasundaram C. Surgical management of peroneal nerve injury in complex sports knee injuries. Clin. Surg. 2016; 1:1008.
Nath RK, Somasundaram C. Gait improvements after peroneal or tibial nerve transfer in patients with foot drop: a retrospective study. ePlasty. 2017; 17:283-293.
Research Objectives
Using innovative new surgical techniques, including nerve transfer, Dr Nath is working to improve the treatment for foot drop and has demonstrated that his approach is a feasible and effective management option for patients with foot drop. Bio Dr Nath serves as a Reconstructive Microsurgeon and as the Director of Texas Nerve and Paralysis Institute at Houston, USA. He received his MD degree in 1988 from Northwestern University, The Feinberg School of Medicine, Chicago. This was followed by internship and residency at Northwestern and at the Department of Surgery in plastic and reconstructive surgery, Washington University in St. Louis, followed by two fellowship years in peripheral nerve injury. He joined the Faculty at Baylor College of Medicine in 1996, and he served there until 2004. Contact Dr Rahul Nath, MD Texas Nerve and Paralysis Institute
6400 Fannin St,
Suite 2420
Houston, TX 77030,
USA
E: Nath@drnathmedical.com
T: +1 (713) 592 9900
W: http://www.drnathclinics.com/
W: http://www.drnathbrachialplexus.com/
W: http://health.usnews.com/doctors/rahul-nath-104165







 Dr Nath serves as a Reconstructive Microsurgeon and as the Director of Texas Nerve and Paralysis Institute at Houston, USA. He received his MD degree in 1988 from Northwestern University, The Feinberg School of Medicine, Chicago. This was followed by internship and residency at Northwestern and at the Department of Surgery in plastic and reconstructive surgery, Washington University in St. Louis, followed by two fellowship years in peripheral nerve injury. He joined the Faculty at Baylor College of Medicine in 1996, and he served there until 2004.
Dr Nath serves as a Reconstructive Microsurgeon and as the Director of Texas Nerve and Paralysis Institute at Houston, USA. He received his MD degree in 1988 from Northwestern University, The Feinberg School of Medicine, Chicago. This was followed by internship and residency at Northwestern and at the Department of Surgery in plastic and reconstructive surgery, Washington University in St. Louis, followed by two fellowship years in peripheral nerve injury. He joined the Faculty at Baylor College of Medicine in 1996, and he served there until 2004.