Lupus is a chronic autoimmune disease, which means that the immune system – the body’s defence system – malfunctions, producing antibodies that attack the body’s own tissues, causing inflammation. Lupus is very different in each individual patient, and this can make it difficult to diagnose. It can cause unpredictable flares of inflammation affecting almost any organ in the body.
Lupus – a multi-system disease
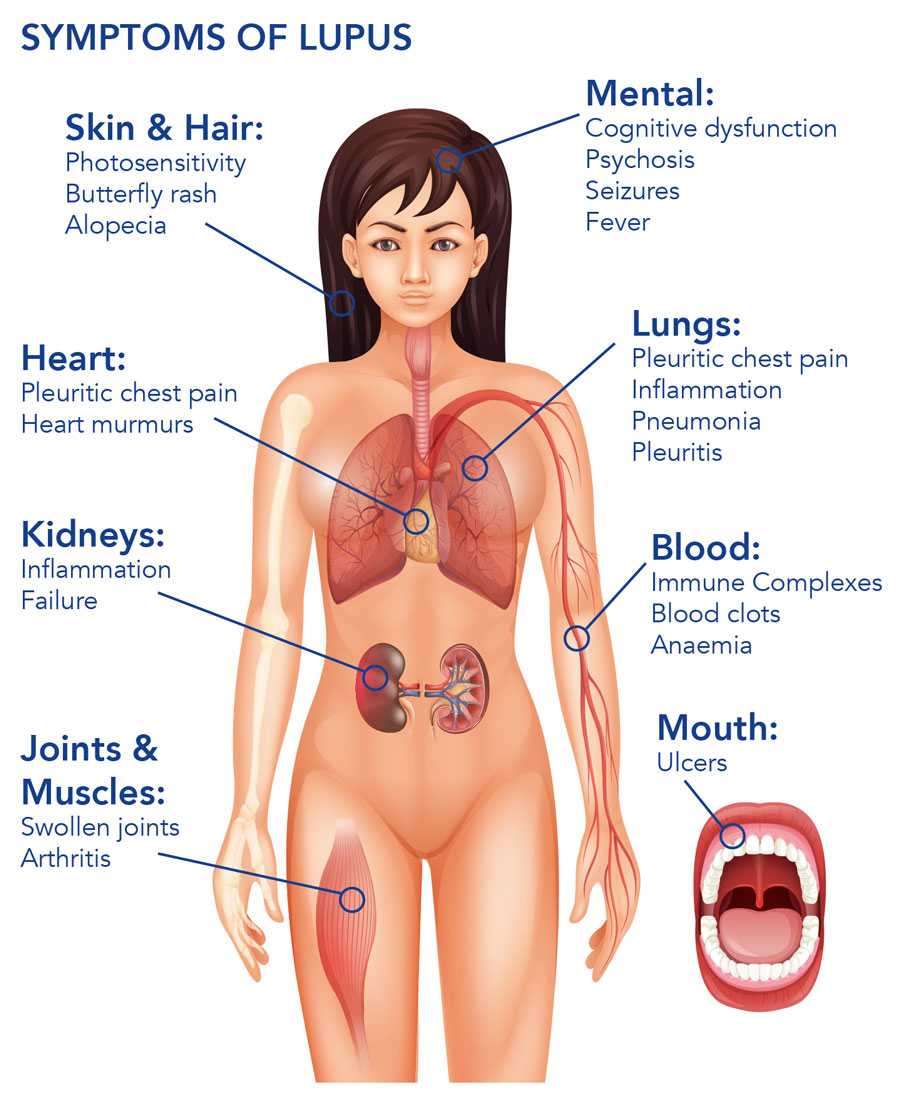
Inflammation caused by lupus often affects the joints and skin, however, in the most common and serious type of lupus – systemic lupus erythematosus (SLE) – inflammation can affect the kidneys, brain, lungs, and blood vessels and can be life-threatening. In 50% of cases, SLE affects the kidneys and is called lupus nephritis (LN). Around a third of SLE patients have signs of LN at the time of their diagnosis, with around 50-60% developing LN during the first 10 years of their disease. A serious condition, the presence of LN reduces survival rates, from 95% to 88% at 10 years.
Lupus that affects the nerves and mental health of patients is called neuropsychiatric SLE (NPSLE). It consists of a broad range of signs and symptoms including cognitive dysfunction, psychosis cerebrovascular disease (where arteries supplying oxygen to the brain are affected), and seizures, and is well documented in patients with established SLE. Up to 90% of adults, adolescents, and children with lupus experience effects of NPSLE at some point in their lives. NPSLE leads to higher risk of hospitalisation and reduced quality of life. In particular, demyelination (damage to the myelin sheath that covers nerve cells and is critical for healthy nerve cell communication) caused by lupus is a rare, life-threatening condition with high risk of disability and death. It’s also thought that blood-brain barrier damage in SLE contributes to the development of the disease, by allowing the development of inflammation-associated agents across the compromised blood-brain barrier.


Treatment
As there is no cure for lupus, appropriate medical intervention is vital to help control the condition. Unfortunately, finding effective treatments poses a major challenge, and standard of care relies on trial and error, generally using treatments for other illnesses that have yet to be assessed for lupus. Effective treatment is especially difficult for patients with LN and NPSLE. First-line treatment includes steroids and immunosuppressants, however, over one-third of patients do not respond to treatment or relapse after initial remission, and the benefits for those who do respond to treatment are often offset by side effects. Committed to helping relieve the burden of disease, the research of Professor Gaetano La Manna and his co-workers at St Orsola Hospital, University of Bologna, Italy are testing alternative standards of care for severe lupus. Their target is the B cells – which play a huge role in the development of lupus disease.

Photo Credit: CC BY-SA 3.0.
The role of B cells
B cells are the immune cells responsible for producing antibodies that attack invading bacteria, viruses, and toxins. B cells are central to the development of disease in systemic lupus erythematosus (SLE). The crucial role of B cells in lupus disease led to the idea that B cell depletion could offer a potential target for therapeutic intervention. Once such anti-B cell therapy is rituximab – an antibody that temporarily depletes B cells. It works by depleting the B cells to reduce inflammation and improve symptoms. Rituximab has been an approved therapy for lymphomas and rheumatoid arthritis since 1997, and in recent years has been prescribed to lupus patients in accordance with several guidelines. This approach is aimed at selectively inhibiting the action of disease without the devastating consequences of unspecific immunosuppression.
As there is no cure for lupus, appropriate medical intervention is vital to help control the condition.

Photo Credit: CC BY-SA 4.0
Rituximab – trials and tribulations
Although there are many clinical reports showing promising results with rituximab therapy for SLE, rituximab treatment shows variability in terms of clinical outcomes. Two large randomised controlled Phase 3 clinical trials, EXPLORER and LUNAR, did not reach their primary endpoints of superior clinical responses compared to placebo for lupus patients. This variability is thought to be a result of both study design and the wide variation of disease in the lupus population.
Despite these disappointing trials, smaller clinical studies show promise for rituximab and report excellent safety profiles for the treatment (superior to current clinical treatment), which fuels its continued use. Rituximab has been shown to be an effective treatment option for patients with severe NPSLE but as yet there have been no randomised controlled trials (the EXPLORER and LUNAR trials excluded patients with severe NPSLE). As a result, the use of rituximab remains limited as a second-line treatment for patients who are resistant to other treatments. For the first time, Professor Gaetano La Manna and his colleagues explored the idea that rituximab could be considered as a first-line treatment, testing its therapeutic potential for severe inflammatory NPSLE. The researchers were especially interested in its use in patients who have high numbers of circulating B cells.

Putting rituximab to the test
In a recently published study, the team reported a 60-year-old woman diagnosed with active SLE and severe neurological damage. She had a severe cognitive impairment – she had a depressed mood, double vision, difficulty pronouncing words, nerve paralysis, weakness and sensory loss in limbs serious kidney damages. The patient also had serious signs of renal damage, demonstrating nephritic syndrome.
Professor Gaetano La Manna and his team prescribed a dose of rituximab in conjunction with corticosteroids and cyclophosphamide (medications that suppress the immune system and decrease inflammation). The patient received four weekly infusions of rituximab (375 g/m2). The treatment successfully lowered inflammation and prevented further damage. Within six months of treatment, the patient’s vision, speech and movement had radically improved. Progressive improvement in nerve damage was seen shortly after the course of treatment, and within one-year, brain damage injury was significantly healed.
The researchers suggest that this therapeutic strategy represents an effective option for severe inflammatory NPSLE, provided it is given with conventional immunosuppressants to reduce the risk of flare and reduce corticosteroid use (which have strong side effects and can induce NPSLE flares).
The patient went into complete remission with no side effects at 36 months. The team suggest that rituximab could be considered as a possible alternative to the standard of care in the management of severe inflammatory NPSLE. Professor Gaetano La Manna et al. say: “We believe, that rituximab could be considered in similar cases, as first-line therapy, especially if the B cell count is high.”
We believe, that rituximab could be considered in similar cases, as first-line therapy, especially if the B cell count is high.
In the 1950s, lupus was a life-threatening condition. Thankfully, due to the introduction of steroids, immunosuppressive drugs and kidney transplantation, most cases are now treatable. But there is still a long way to go. Striving to further improve outcomes and decrease morbidity and mortality in SLE, the team’s research shows potential for rituximab as a first-line treatment for severe lupus. Their research could pave the way for reducing the damaging effects of SLE, improving chances for patients to enjoy a better quality of life.
Treatment of SLE, particularly cases of refractory disease, still poses a major challenge for physicians. The actual clinical efficacies of B-cell-related therapy by rituximab is still undergoing advanced trial studies, however, evidence of rituximab resistance in patients with multidrug-resistant renal disease are reported, increasing the need for additional therapies. Promising experiences, not in SLE but in different renal disease, suggested ofatumumab, alternative anti-CD20 antibodies, as an effective agent in treating rituximab-resistant nephrotic syndrome, however, data is still unavailable in SLE. Therefore, alternative anti-CD20 antibodies may be more consistently effective in SLE treatment, thus several ongoing trials are needed for these issues.
References
- Hickman RA, Hira-Kazal R, Yee CS, Toescu V, Gordon C. (2015). ‘The efficacy and safety of rituximab in a chart review study of 15 patients with systemic lupus erythematosus’. Clin Rheumatol. 34:263–271.
- Fernandez-Nebro A, De La Fuente JL, Carreno L, Izquierdo MG, Tomero E, et al. (2012). ‘Multicenter longitudinal study of B-lymphocyte depletion in refractory systemic lupus erythematosus: The LESIMAB study’. Lupus. 21:1063–1076.
- Cravedi P, Remuzzi G, Ruggenenti P. (2014). ‘Rituximab in primary membranous nephropathy: First-line therapy, why not?’. Nephron Clin Pract, 28:261–269.
- Hahn BH, McMahon MA, Wilkinson A, Wallace WD, Daikh DI, et al. (2012). ‘American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis’. Arthritis Care Res (Hoboken), 64:797–808.
- Iwata S, Tanaka Y. (2016). ‘B-cell subsets, signaling and their roles in secretion of autoantibodies’. Lupus 2016, 25:850–856.
Professor La Manna and his research team aim to discover and create a more effective treatment for lupus disease and improve patients’ quality of life.
Collaborators
- Andrea Angeletti MD, PhD Student, Department of Experimental Diagnostic and Specialty Medicine (DIMES), Nephrology, Dialysis and Renal Transplant Unit, St Orsola Hospital, University of Bologna, Bologna, Italy.
- Giorgia Comai MD, PhD, Department of Experimental Diagnostic and Specialty Medicine (DIMES), Nephrology, Dialysis and Renal Transplant Unit, St Orsola Hospital, University of Bologna, Bologna, Italy.
- Olga Baraldi, MD, PhD, Department of Experimental Diagnostic and Specialty Medicine (DIMES), Nephrology, Dialysis and Renal Transplant Unit, St Orsola Hospital, University of Bologna, Bologna, Italy.
- Anna Laura Croci Chiocchini MD, PhD Student, Department of Experimental Diagnostic and Specialty Medicine (DIMES), Nephrology, Dialysis and Renal Transplant Unit, St Orsola Hospital, University of Bologna, Bologna, Italy.
- Paolo Cravedi MD, PhD, Department of Medicine, Division of Nephrology, Icahn School of Medicine at Mount Sinai, USA.
Bio
 Professor La Manna received his PhD in Nephrology at the University of Bologna in 1995. He then went on to complete his post-doctorate degree in Medical Science at the University of Bologna in 1997. Prof La Manna currently works as Director of the Nephrology, Dialysis and Renal Transplantation Unit at the S. Orsola-Malpighi University Hospital of Bologna.
Professor La Manna received his PhD in Nephrology at the University of Bologna in 1995. He then went on to complete his post-doctorate degree in Medical Science at the University of Bologna in 1997. Prof La Manna currently works as Director of the Nephrology, Dialysis and Renal Transplantation Unit at the S. Orsola-Malpighi University Hospital of Bologna.
Contact
Professor Gaetano La Manna
U.O. Nefrologia Dialisi e Trapianto
Renale, Pad 15
Ospedale Sant’Orsola
Via Massarenti 9,
Bologna, Italy
E: gaetano.lamanna@unibo.it
T: +39 328 414 0532
Facebook: www.facebook.com/SinReni/
Facebook: www.facebook.com/PoliclinicoDiSantOrsola/